Printable Blank Authorization To Release Information Form - Web a medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Web authorization to disclose health information; Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care. Web to request release of medical information please complete and sign this form i,. Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent.

10 Authorization To Release Information Form Template Template Free Download
Web to request release of medical information please complete and sign this form i,. Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care. Web authorization to disclose health information; Web a medical records release authorization form is a.

Release of Information Template Fill Out and Sign Printable PDF Template signNow
Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web to request release of medical information please complete and sign this form i,. Web authorization to disclose health.

Blank Authorization to Release Information Form Fill Out and Sign Printable PDF Template signNow
Web to request release of medical information please complete and sign this form i,. Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of.

FREE 13+ Sample Release of Information Forms in PDF MS Word
Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care. Web authorization to disclose health information; Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web a.

Generic Authorization to Release Medical Records Form Download the free Printable Basic Blank
Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web to request release of medical information please complete and sign this form i,. Web authorization to disclose health.

Release Of Information Forms Printable (BLANK TEMPLATE)
Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care. Web authorization to disclose health information; Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web to.

Blank Authorization To Release Information Form Fill Online, Printable, Fillable, Blank
Web authorization to disclose health information; Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web a medical records release authorization form is a document that allows a.
FREE 8+ Sample Release Of Information Forms in PDF MS Word
Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web to request release of medical information please complete and sign this form i,. Web a medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Web if this.

FREE 9+ Sample Release of Information Forms in MS Word PDF
Web to request release of medical information please complete and sign this form i,. Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care. Web we have developed a printable blank authorization to release information form that can be.

Consent To Release Information Form Template DocTemplates
Web to request release of medical information please complete and sign this form i,. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web authorization to disclose health information; Web if this form is being completed by a person with legal authority to act an individual’s behalf, such.
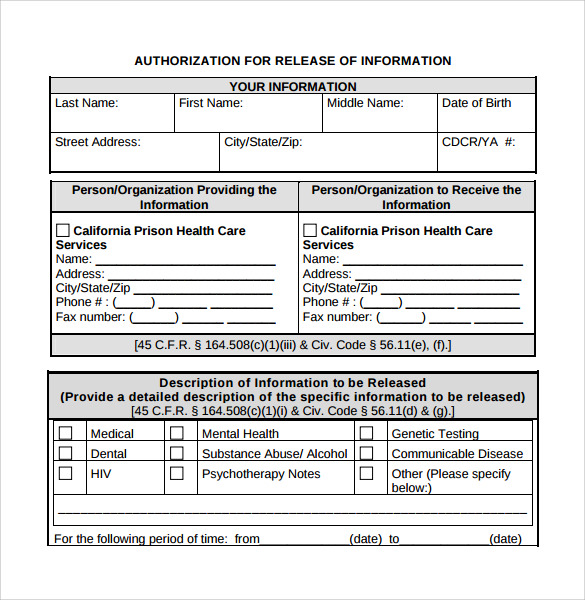
Web to request release of medical information please complete and sign this form i,. Web authorization to disclose health information; Web we have developed a printable blank authorization to release information form that can be an alternative to the hipaa. Web a medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care.
Web Authorization To Disclose Health Information;
Web to request release of medical information please complete and sign this form i,. Web if this form is being completed by a person with legal authority to act an individual’s behalf, such as a parent or legal guardian of a minor or health care. Web this form should include specific details such as the person or organization being authorized, the person or organization being sent. Web a medical records release authorization form is a document that allows a person to disclose protected health information to a third party.